Scarlet fever : Dick and Schultz-Charlton tests, active and passive immunity / by R.A. O'Brien.
- O'Brien, Richard Alfred, 1878-1970.
- Date:
- [1926?]
Licence: In copyright
Credit: Scarlet fever : Dick and Schultz-Charlton tests, active and passive immunity / by R.A. O'Brien. Source: Wellcome Collection.
1/2
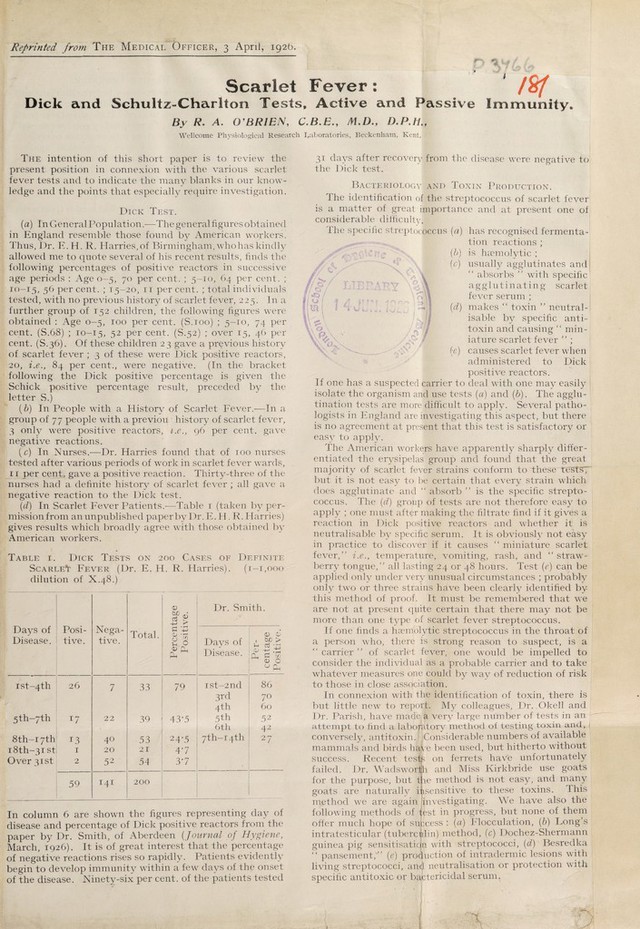
![Reprinted from The Medical Officer, 3 April, 192b. Scarlet Fever : ' W Dick and Schultz-Charlton Tests, Active and Passive Immunity, By R. A. O’BRIEN, C.B.E., M.D., D.P.H., Wellcome Physiological Research Laboratories, Beckenham, Kent. The intention of this short paper is to review the present position in connexion with the various scarlet fever tests and to indicate the many blanks in our know¬ ledge and the points that especially require investigation. Dick Test. (a) In General Population.-—The general figures obtained in England resemble those found by American workers. Thus, Dr. E. H. R. Harries, of Birmingham, who has kindly allowed me to quote several of his recent results, finds the following percentages of positive reactors in successive age periods : Age 0-5, 70 per cent. ; 5-10, 64 per cent. ; 10-15, 5^ Per cent. ; 15—20, 11 percent. ; total individuals tested, with no previous history of scarlet fever, 225. In a further group of 152 children, the following figures were obtained : Age 0-5, 100 per cent. (S.100) ; 5-10, 74 per cent. (S.68) ; 10-15, 52 per cent. (S.52) ; over 15, 46 per cent. (S.36). Of these children 23 gave a previous history of scarlet fever ; 3 of these were Dick positive reactors, 20, i.e., 84 per cent., were negative. (In the bracket following the Dick positive percentage is given the Schick positive percentage result, preceded by the letter S.) (b) In People with a History of Scarlet Fever.—In a group of 77 people with a previou history of scarlet fever, 3 only were positive reactors, i.e., 96 per cent, gave negative reactions. (c) In Nurses.—Dr. Harries found that of 100 nurses, tested after various periods of work in scarlet fever wards, II per cent, gave a positive reaction. Thirty-three of the nurses had a definite history of scarlet fever ; all gave a negative reaction to the Dick test. (d) In Scarlet Fever Patients.—Table 1 (taken by per- missionfrom an unpublished paper by Dr. E. H. R. Harries) gives results which broadly agree with those obtained by American workers. Table i. Dick Tests on 200 Cases of Definite Scarlett Fever (Dr. E. H. R. Harries). (1-1,000 dilution of X.48.) Days of Disease. Posi¬ tive. Nega¬ tive. Total. Percentage Positive. Dr. Sm Days of Disease. Per- 7 centage Positive. ist~4th 26 7 33 79 ist-2nd 86 3rd 70 4th 60 5th-7th *7 22 39 43-5 5th 52 6th 42 8th-i7th 13 40 53 24-5 7th-i4th 27 i8th-3ist 1 20 21 47 Over 31st 2 52 54 37 . 59 141 200 In column 6 are shown the figures representing day of disease and percentage of Dick positive reactors from the paper by Dr. Smith, of Aberdeen [Journal of Hygiene, March, 1926). It is of great interest that the percentage of negative reactions rises so rapidly. Patients evidently begin to develop immunity within a few days of the onset of the disease. Ninety-six per cent, of the patients tested 31 days after recovery from the disease were negative to the Dick test. Bacteriology and Toxin Production. The identification of the streptococcus of scarlet fever is a matter of great importance and at present one of considerable difficulty] The specific streptococcus (a) has recognised fermenta¬ tion reactions ; (b f/ / li cs (s) (d) V) is haemolytic ; usually agglutinates and “ absorbs ” with specific a g g 1 u t i n a t i n g scarlet fever serum ; makes “ toxin ” neutral- isable by specific anti¬ toxin and causing “ min¬ iature scarlet fever ” ; causes scarlet fever when administered to Dick positive reactors. If one has a suspected carrier to deal with one may easily ; isolate the organism and use tests (a) and (b). The agglu¬ tination tests are more difficult to apply. Several patho¬ logists in England are investigating this aspect, but there is no agreement at present that this test is satisfactory or easy to apply. The American workers have apparently sharply differ¬ entiated the erysipelas group and found that the great majority of scarlet fever strains conform to these test ST but it is not easy to be certain that every strain which does agglutinate and “ absorb ” is the specific strepto¬ coccus. The (d) group of tests are not therefore easy to apply ; one must after making the filtrate find if it gives a reaction in Dick positive reactors and whether it is neutralisable by specific serum. It is obviously not easy in practice to discover if it causes “ miniature scarlet fever/’ i.e., temperature, vomiting, rash, and “ straw¬ berry tongue,” all lasting 24 or 48 hours. Test (e) can be applied only under very unusual circumstances ; probably only two or three strains have been clearly identified by this method of proof. It must be remembered that we are not at present quite certain that there may not be more than one type of scarlet fever streptococcus. If one finds a haemolytic streptococcus in the throat of a person who, there is strong reason to suspect, is a “ carrier ” of scarlet fever, one would be impelled to consider the individual as a probable carrier and to take whatever measures one could by way of reduction of risk to those in close association. In connexion with the identification of toxin, there is but little new to report. My colleagues, Dr. .Okeil and Dr. Parish, have made; a very large number of tests in an attempt to find a laboratory method of testing toxin and, 1 conversely, antitoxin. Considerable numbers of available mammals and birds have been used, but hitherto without success. Recent tests on ferrets have unfortunately failed. Dr. Wadsworfjh and Miss Kirkbride use goats ie method is not easy, and many insensitive to these toxins. This method we are again investigating. We have also the following methods of test in progress, but none of them offer much hope of success : (a) Flocculation, (b) Long’s intratesticular (tuberculin), method, (c) Dochez-Shermann guinea pig sensitisation with streptococci, id) Besredka “ pansement/’ (e) production of intradermic lesions with living streptococci, aiM neutralisation or protection with specific antitoxic 07 bactericidal serum. for the purpose, but t goats are naturally again.](https://iiif.wellcomecollection.org/image/b30625920_0001.jp2/full/800%2C/0/default.jpg)