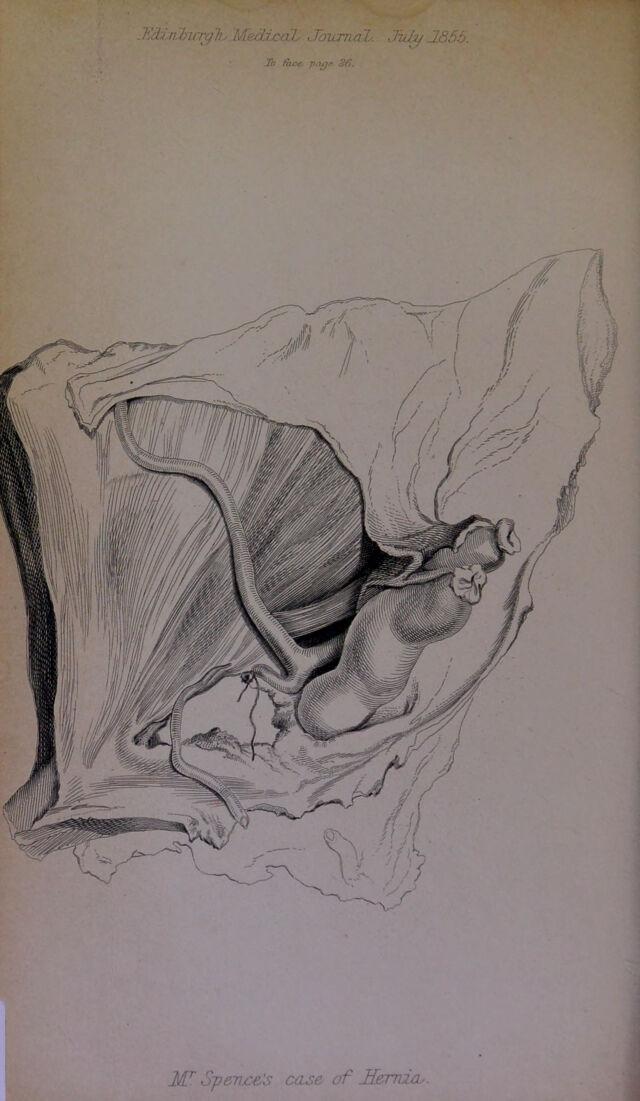
Case of femoral hernia, containing the caput coecum, and complicated with an irregular obturator artery surrounding and constricting the protrusion, and other cases illustrative of the operation for femoral hernia / by James Spence.
- James Spence
- Date:
- 1855
Licence: Public Domain Mark
Credit: Case of femoral hernia, containing the caput coecum, and complicated with an irregular obturator artery surrounding and constricting the protrusion, and other cases illustrative of the operation for femoral hernia / by James Spence. Source: Wellcome Collection.
Provider: This material has been provided by The Royal College of Surgeons of England. The original may be consulted at The Royal College of Surgeons of England.
15/18 page 13
![Hemarks.—The first fiveof tliese cases form a group having some features in common. The patients were all females, debilitated either by old age or by previous disease. The general symptoms present, the length of time these had existed, the tightness of the sti’icture, the morbid alteration in the constricted portion of bowel in all, and the feculent vomiting and hiccough in some of them— were elements for an unfavourable prognosis; and yet in none of them did any unfavourable symptoms supervene. In a former series of hernia cases, published in the Monthly Journal, Wvd(\. occasion to contrast different cases,, and to remark on the difficulty of prognosis from the appearance of the constricted ])ortion of intestine; but experience leads me to believe, that examination of the state of the bowel immediately above the con- striction may form a criterion. If it be of a j)ale reddish-grey colour, and feel thick and fleshy, the chances are in favour of a successful result, the constricted portion will be likely to recover itself when replaced. On the other hand, if the bowel above the constriction be of a bright ))ink colour, appearing thin and as if distended with air, and bedewed with a clammy exudation,—and if there be a large escaj)e of red or dark-colourecl serous fluid from the abdomen on dividing the constriction,—the prognosis is most imfavourable, as indicating that peritonitis has commenced, or that structural alteration is ])ro- cecding, in and beyond the constricted portion. The practice of gently drawing down and examining an inch or two of the bowel above the constriction, is advisable, 1 think, in all cases where we open the sac, both because it ensures that the con- striction is fairly removed, and, by allowing the j)rotrusion to be emptied of its contents, renders its reduction more easy; but it is specially necessary where the constriction has been of long dura- tion, for ill such cases perforation not unfrequently occurs from half- an-inch to an inch above the constriction. I have in my possession three preparations showing this state in cases of femoral hemia where the jiatients died without being operated on, and 1 need hardly I’emark what would be the result of returning a jiortion of bowel either actually jierforated or about to sphacelate. Some of the cases nairated also jiresent individual peculiarities deserving attention.^ Thus, in Mrs W.’s case, we find a condition showing the necessity for constant caution in every case of hernio- tomy, however simple the case may seem ; for here, when the lower part of the sac was opened over the collected fluid, had 1, without further examination, attempted to run the bistoury upwards to slit it open, the bowel, from its close adhesion above, would almost cer- tainly have been injured, and this has actually happened in similar cases. In Margaret C.’s case, the congested lymphatic glands adherent to the sac, and enveloped in the thin, smooth, transparent fascia pro])na, had very much the appearance of the sac itself. 1 have met](https://iiif.wellcomecollection.org/image/b22368504_0017.jp2/full/800%2C/0/default.jpg)