Feebleness of growth and congenital dwarfism : with special reference to dysostosis cleido-cranialis / by Murk Jansen.
- Jansen, Murk, 1867-1935.
- Date:
- 1921
Licence: In copyright
Credit: Feebleness of growth and congenital dwarfism : with special reference to dysostosis cleido-cranialis / by Murk Jansen. Source: Wellcome Collection.
88/108 page 70
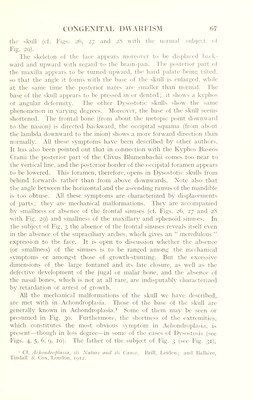
![small, enhances the normal infolding of the embryo in the fifth or sixth week of embryonic life; that it at the same time increases hydrostatic pressure inside the amniotic sac and squeezes the blood out of the foetus during the formation of its cartilaginous skeleton. We will now try to prove that all the symptoms of Dysostosis may be explained in an equally simple way, if we assume that smallness of the amnion infolds the foetus during the eighth week of fcvtal life. Whilst in Achondroplasia we observe only one infolding of the embryo, viz. the infolding of the embryonic axis, in Dysostosis Cleido-cranio-(digitalis) we observe two infoldings : one of the foetal axis, another infolding of the transverse axis which passes through the shoulders. Our conception is as follows : If in the eighth Week the amnion remains too small, by direct pressure it brings the forehead of the foetus into too intimate contact with the anterior surface of the trunk. The shoulders are displaced forward and squeezed against the ribs and eventually also the inferior part of the head. The clavicles (sometimes also a single clavicle) are folded. So direct pressure explains all the mechanical malformations wre have enumerated, and even a number of others, such as the frequent depression shown by the sternum, and probably also the abnormal curve of the shoulder- blade and of the acromion, as well as the subluxation of the humerus which have been described. If we apply the principles mentioned in the Introductory Note to the symptoms of retardation of growth in Dysostosis Cleido-cranio-(digitalis) which we have just enumerated, they at once lose their enigmatic character. In the eighth week of foetal life all parts which in Dysostosis are affected by retardation of development—the frontal bones, the clavicles, the intermediate and terminal phalanges of the toes—are still flexible, scleroblastematous or precartilaginous; but at the same time they are changing their consistency by becoming osseous (frontal bones, clavicles) or cartilaginous (intermediate and terminal phalanges). So they are all in a condition of rapid growth. Whilst all other skeletal parts have just undergone this important change, these bones are at that time the only ones that change their consistency; hence also the only ones whose rapidity of growth determines enhanced vulnerability. The fibrous covering of the brain is ossifying at the moment of infolding. The medial part of the forehead, prominent as it naturally is, must meet with the greatest pressure from the trunk. [The back part of the head, though meeting writh the same direct pressure of the amniotic sac, dis¬ tributes this pressure over a much larger area (cf. Postscript, last paragraph p. 82).] For the same reason the jugal or malar bones, forming a prominence, are more exposed than the surrounding parts. The skin](https://iiif.wellcomecollection.org/image/b29812240_0088.jp2/full/800%2C/0/default.jpg)



 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image