In the early 20th century, a new form of treatment for tuburculosis emerged in Europe and North America. Sanatoriums were a hybrid between a hospital and a resort, built to maximise patients’ exposure to sunlight and clean air. Their bright, open spaces influenced both healthcare and modern architecture. But a darker aspect of sanatorium care, as Sadie Levy Gale discovered, was the extent to which TB patients were monitored and policed during their stay.
The history of sanatoriums and surveillance
Words by Sadie Levy Gale
- In pictures

1 of 10
In the 19th century, tuberculosis (TB) was known as the “romantic disease”, and vaunted as a sign of an artistic sensibility. The convalescent consumptive was a staple of Victorian literature and art, often because many famous writers and artists suffered from tuberculosis themselves. But in reality, the effect of the disease on mortality rates was far from picturesque: four million people died of TB in England and Wales between 1851 and 1910. Before the discovery of antibiotics, doctors believed that a regimen consisting of exposure to the open air at high altitudes, a cold climate, hygiene education and isolation was the most effective treatment.
2 of 10
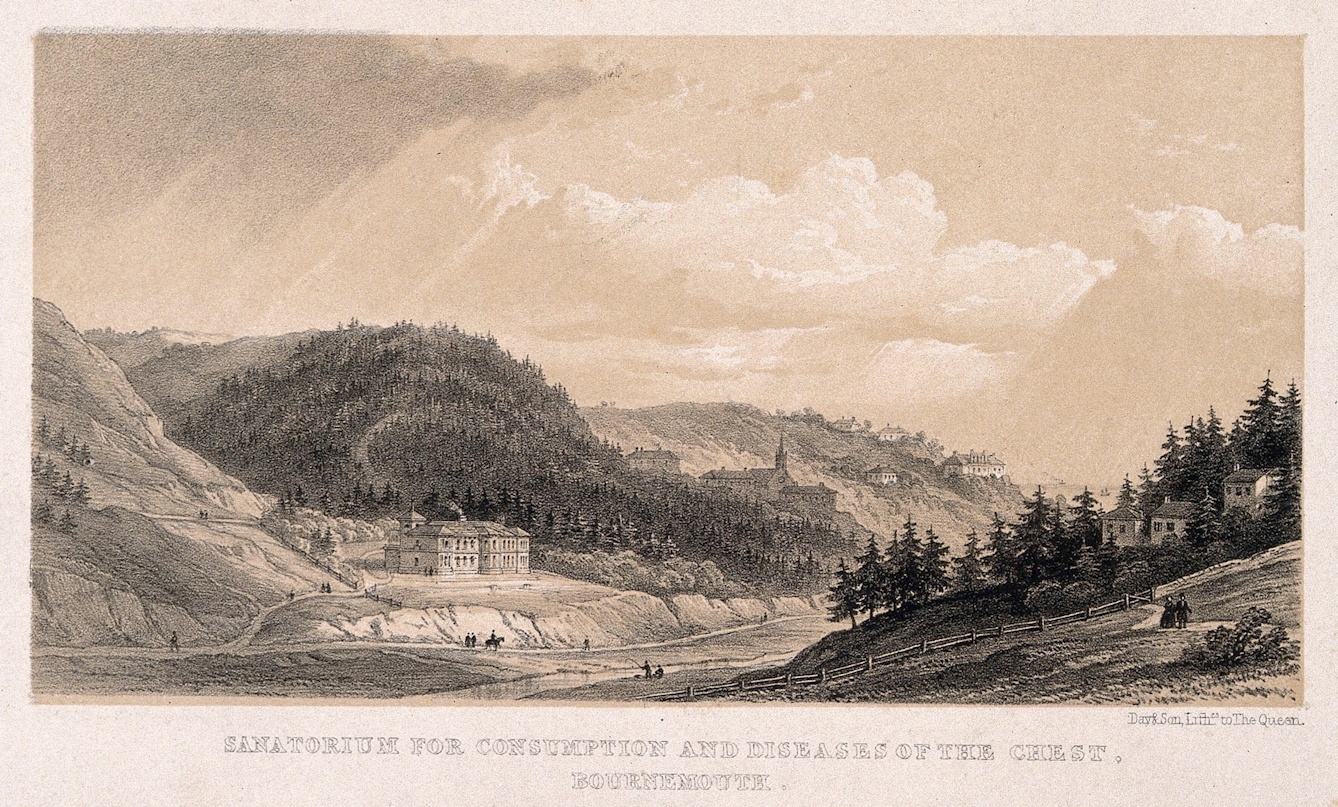
At the heart of this approach was the belief that foul air caused tuberculosis. Despite Robert Koch’s discovery of the TB germ, Mycobacterium tuberculosis in 1882, the foul-air theory continued to shape 20th-century treatments. The high premium placed on ‘pure’ air as a therapeutic tool informed the growth of specialised hospitals known as sanatoriums. These were situated in rural locations to maximise the exposure of patients to sunlight and fresh air, but also to segregate them from the general population. The sanatorium movement had spread to every continent in the world by the mid-20th century. The fir trees, unpopulated hills and vast skies surrounding this sanatorium near Bournemouth exemplify what was believed to be the ideal therapeutic landscape for tuberculosis.

3 of 10
While the first sanatoriums tended to be repurposed country houses or work hospitals, by the 1920s purpose-built buildings with architectural features that enhanced exposure to sunlight and fresh air were being built. Sun-balconies (also known as ‘solariums’), large, glazed windows and flat roofs were typical design features of sanatoriums that would also become hallmarks of Modernist architecture. The quality of the sanatorium, and the treatment offered, varied according to the wealth of the patients. More exclusive sanatoriums were hybrids between a hospital and a resort, while others were far more spartan, like this sanatorium in the English West Midlands.

Rest hour ; Mont Alto Sanatorium, Pennsylvania. Source: Wellcome Collection. © Credit: Mont Alto Sanatorium for tuberculosis, Pennsylvania: male patients are shown sitting in deckchairs in the open air, during 'rest hour'. Photograph, 1920/1940?..
4 of 10
The architecture of purpose-built sanatoriums enabled doctors and nurses to monitor patients more closely – the transparent, open-air designs normalised a disciplinarian regime of surveillance, which was a defining feature of tuberculosis treatment in the late 19th and early 20th centuries. From morning to evening, every minute of a patient’s day was regulated: doctors decided what patients ate, how long they were to sleep, and planned mandatory physical exercises and rest periods. In some institutions, patients weren’t even allowed to read or write, as it was thought this could interfere with developing strong “mental hygiene”. In this photograph of Mont Alto Sanatorium in Pennsylvania, USA, male patients can be seen in deckchairs during “rest hour”, under the close surveillance of the doctor.

5 of 10
Tuberculosis hospitals with spacious grounds often featured ‘chalets’ designed to accommodate patients. Little more than timber huts (that supposedly referenced European health resorts), chalets were used to increase the amount of pure air tuberculosis patients breathed. Isolating patients not only segregated those who were sick and recovering, it also enabled new treatments and cures to be tested. Patients were required to spend extended periods of time in the chalets through winter or summer – some sanatoriums even equipped sufferers with snow-proof blankets. Life in the chalets was lived under the continuous observation of a doctor or nurse.

A healthy boy, protected from tuberculosis by fresh air and exercise., Colour lithograph by André Wilquin, 1942.. Source: Wellcome Collection. © Credit: A healthy boy, protected from tuberculosis by fresh air and exercise. Colour lithograph by André Wilquin, 1942..
6 of 10
Once patients were deemed to be sufficiently recovered, they were required to participate in outdoor exercise drills that took place in all seasons. Militaristic in nature, these exercise regimens aimed to test and improve the strength of the body and character, enabling patients to build up resistance to tuberculosis and perhaps eliminate it altogether. As this French public health poster shows, patients wore as little clothing as possible, in order to benefit from the therapeutic effects of sunshine and fresh air.

Rest hour ; Mont Alto Sanatorium, Pennsylvania. Source: Wellcome Collection. © N.Y. [New York] : Apeda Pictures, [1920/1940?].
7 of 10
Mandatory exercise went hand in hand with the imposition of “graduated labour” at many sanatoriums. In the early 20th century, prominent doctors like Dr Robert Philip, a pioneer in the treatment of tuberculosis, believed that providing work for patients was vital to their successful reintegration into society. Writing in the British Medical Journal in 1906, Philip declared: “My idea of a sanatorium for the working class is that of a busy hive… a kind of working colony.” The enforcement of labour at charitable or public sanatoriums was framed as therapeutic, but in reality, it followed the discipline of reform institutions like the workhouse and was only required of working-class patients.
8 of 10
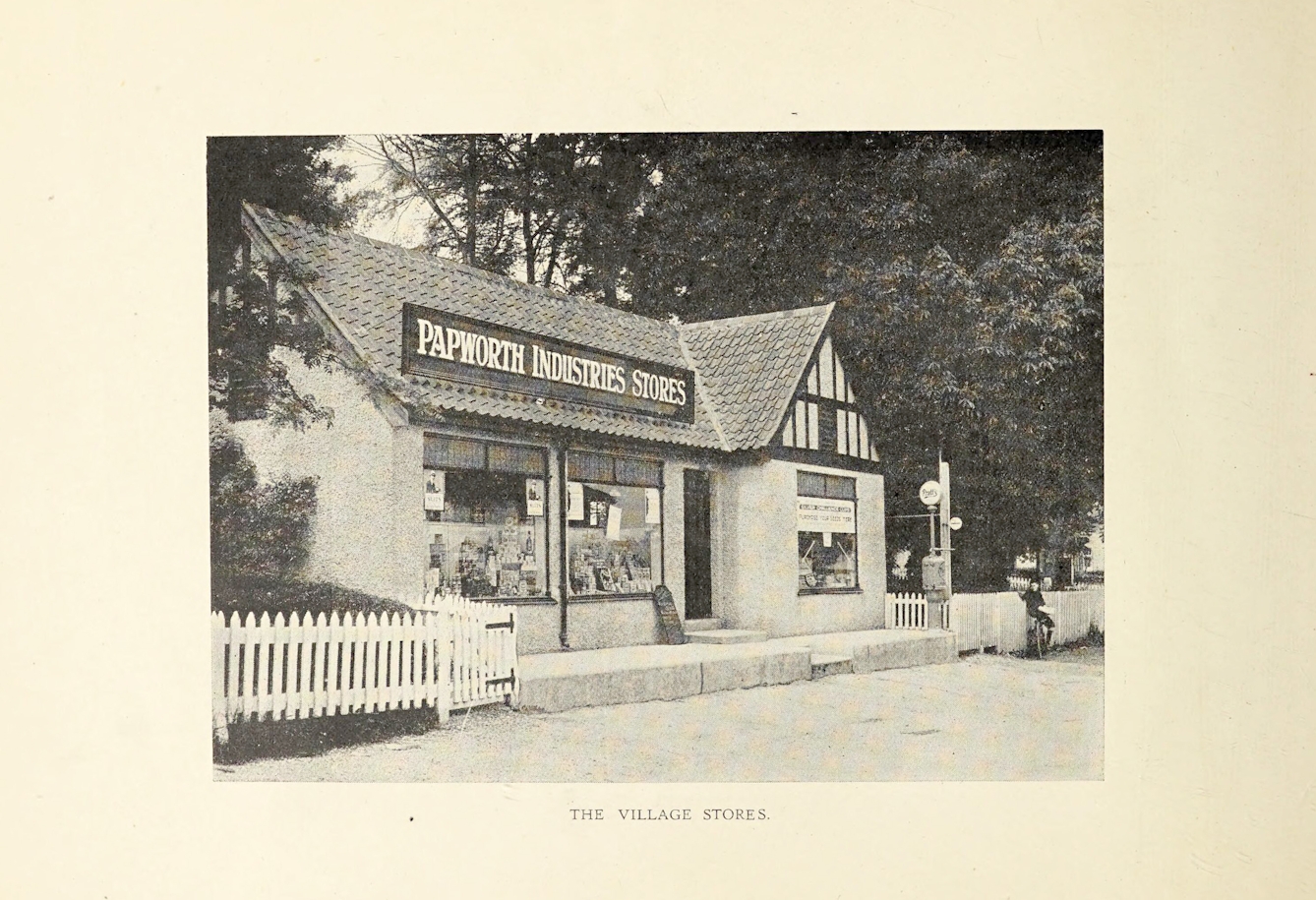
In the early 20th century, tuberculosis ‘colonies’ began to emerge as a form of comprehensive treatment, in which housing, employment and leisure facilities were provided on-site. Papworth Hall Colony in Cambridgeshire, founded by Dr Pendrill Varrier-Jones in 1917, was the largest and most famous of these settlements. At Papworth, patients in recovery were encouraged to work in on-site factories, and the most healthy patients lived in cottages with their families. Some patients stayed in the colony for the rest of their lives, offering an unprecedented opportunity for doctors to observe their patients long-term. Dr Varrier-Jones believed that the tuberculous person’s “whole life, waking, working, sleeping and all the manifold activities of existence [should] be carefully guarded and guided”.
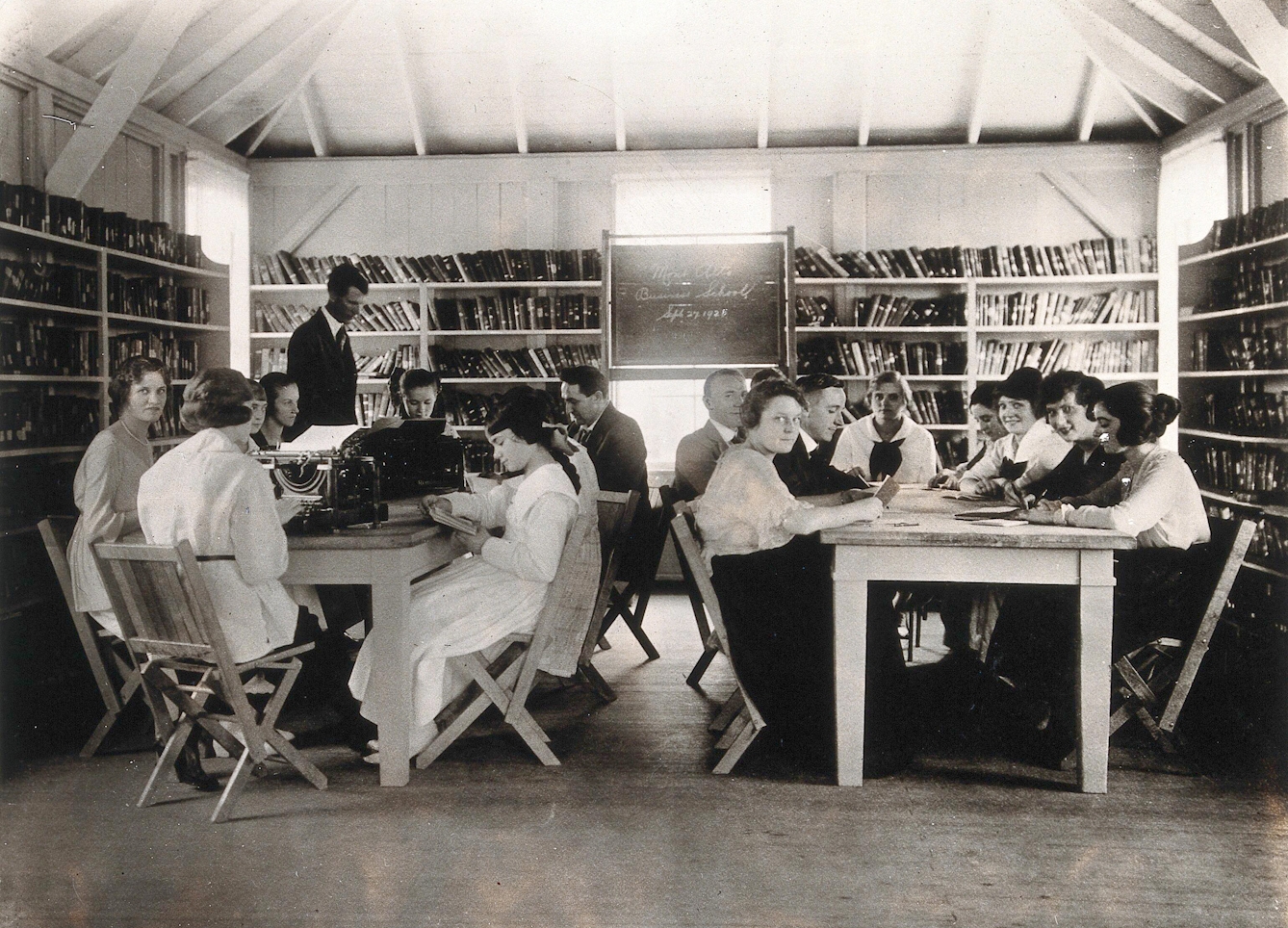
Many patients at the state sanatoria come from the congested & foreign quarters of the big cities. This is an "Americanization" class. 1925. Source: Wellcome Collection. © Credit: Mont Alto Sanatorium for tuberculosis, Pennsylvania: an 'Americanization' class for adult patients of non-American origin. The patients are shown seated around tables in a schoolroom, reading and typing. Photograph, 1925..
9 of 10
By the turn of the century, tuberculosis began to be perceived as a disease of the urban working classes who suffered from the effects of industrialisation, rather than a middle-class affliction. Socio-economic disparities that put populations at high risk of infection, such as overcrowding and malnutrition, disproportionately affected racial- and ethnic-minority groups. This photograph shows an ‘Americanisation’ class for immigrants with TB taking place at Mont Alto Sanatorium in 1925. The accompanying caption, “many patients at the state sanatoria come from congested & foreign quarters of the big cities”, implies a connection between foreign bodies, poor hygiene and ill health. The ‘Americanisation’ class reveals how sanatoriums also functioned as mechanisms of control, in which ‘undesirable’ or even ‘dangerous’ individuals could be reformed by the institution.

Throat treatment - helio ; Cressan State Sanatorium - Pennsylvania. Source: Wellcome Collection. © Credit: Helio throat treatment, Cresson Sanatorium, Pennsylvania: a nurse is shown watching two tuberculosis patients holding out their tongues, while sunlight is reflected into their mouths by means of small mirrors (?). Photograph, 1920/1940?..
10 of 10
By the 1950s, the widespread use of TB vaccination, coupled with the rise of mass-produced pharmaceuticals, made the spatial segregation of TB patients redundant. The sanatorium ‘cure’ had been in question for some years by this point – while sanatoriums reduced the risk of tuberculosis spreading to uninfected people, 50 per cent of those who entered a sanatorium died within five years. Many of their treatments, such as heliotherapy (shown here being used to ‘kill’ TB bacteria with sunshine), had proven ineffective. Most sanatoriums were gradually demolished or repurposed, yet an element of surveillance in TB treatment remains to this day. Directly observed therapy (DOT) is a widely practised method for ensuring that TB patients complete their course of treatment. In DOT a health worker observes the patient taking each dose in order to ensure that they complete the full course of treatment. The method is not without controversy, as it tends to focus on "under-served groups”, which in practice generally means monitoring the homeless, vulnerable migrants, prisoners and people who misuse substances.
About the author

Sadie Levy Gale
(she/her)
Sadie Levy Gale is a PhD student at Cardiff University’s school of Journalism, Media and Culture. Her research focuses on healthcare, the built environment and national identity in 20th-century British photojournalism.