For centuries women gave birth in the familiar environment of home, surrounded and supported by women they knew. Tania Staras, an expert in the history of maternity care, tracks the developments that heralded the involvement of men and led to the increasing medicalisation of birth.

1 of 11
Historically, birth was a domestic event, not a medical one. This means that women of all social classes laboured and birthed at home surrounded by friends and family. As this Dutch picture from the 17th century shows, women were supported by other women when they laboured – these women are celebrating the safe arrival of the baby while the mother rests in bed. If one of the women was considered skilled in supporting birth, she would have been described as a midwife (‘midwife’ in Old English means ‘with woman’ and the term was used from the 14th century). Male doctors and medicine rarely played a part in birth.

2 of 11
From the 17th century onwards, midwives had competition from male doctors. Instruments such as forceps were developed by doctors to manage difficult births. These types of births were very rare, but doctors were increasingly sent for when there was an emergency. Midwives did not use instruments to manage births and they rarely used medicines – they focused on support. This picture shows the female midwife with cosy hearth and baby feeding bottle and the male doctor, who was beginning to take her place, with his instruments and potions. Doctors charged more money than midwives, so by the early 19th century they were becoming a fashionable choice for wealthy families.

3 of 11
Nowadays we expect complex pregnancies and difficult births to be managed in hospital. Before the 20th century, however, nearly all births took place at home, regardless of their challenges. This engraving shows a labouring woman supported by her husband and a midwife. Another attendant washes a newly delivered baby. The woman in this picture is having twins – the first has been born, the second yet to arrive. Midwives, and, increasingly, doctors, were skilled in managing situations such as twin or breech births in the domestic setting.
4 of 11
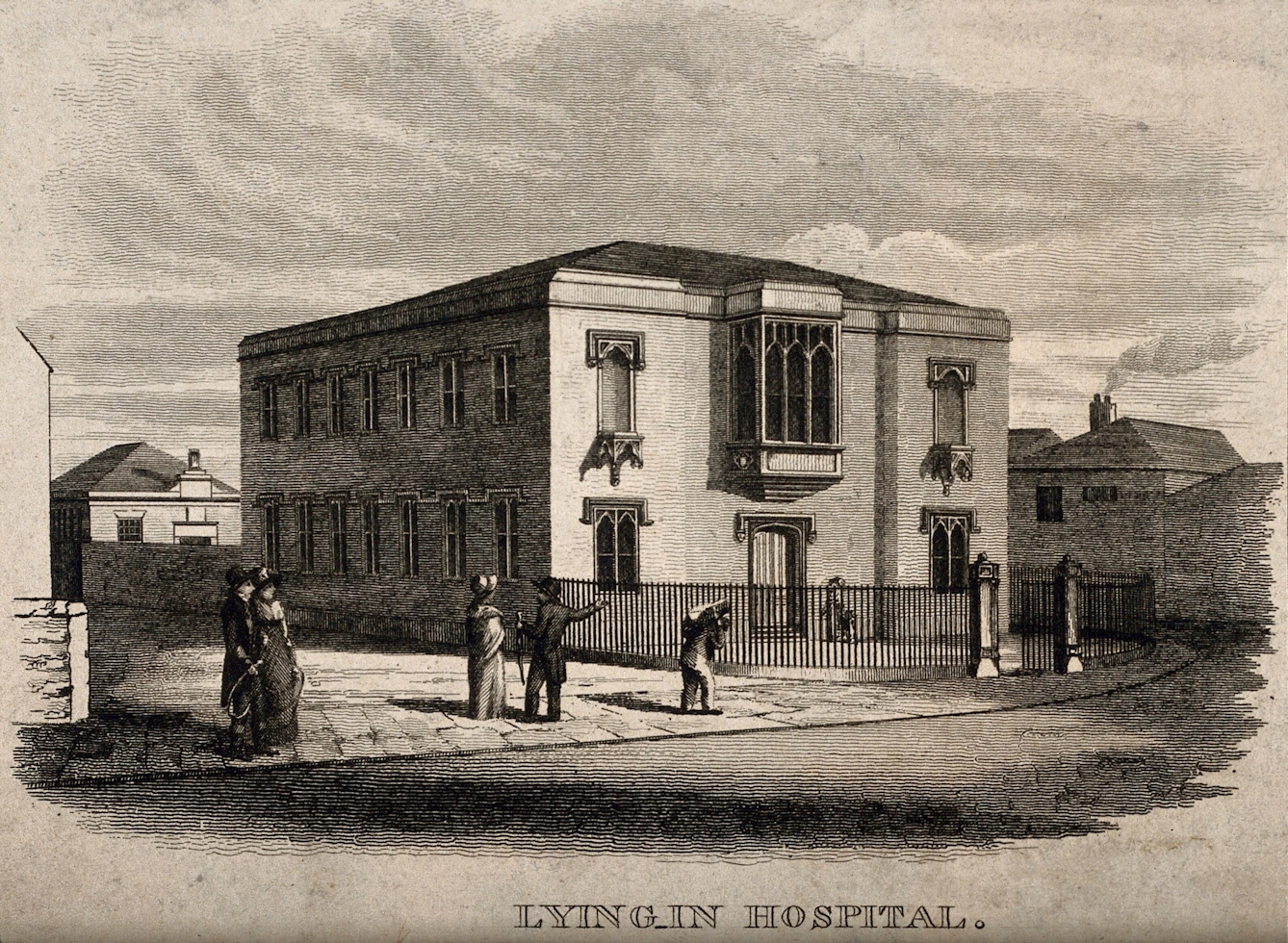
This sturdy-looking building represents the beginning of a fundamental change in beliefs about the best place to give birth – although the change took a long time to become reality. In the decades around 1800, ‘lying-in’ hospitals began to spring up in cities across the UK. They were championed by doctors who felt it would be cheaper and more effective to look after labouring women if they all gave birth in the same place. Early lying-in hospitals had very mixed fortunes, though. In the days before antibiotics and antiseptics, they were a breeding ground for the development and spread of infectious diseases. Many hospitals closed down after outbreaks of puerperal fever, which had a very high mortality rate for newly delivered women. For most of the Victorian period, hospitals were seen as far more dangerous places to give birth than home.

5 of 11
In the early decades of the 20th century, most women still gave birth at home with a midwife in attendance. After the 1902 Midwives Act was passed in England and Wales, midwives had to be trained and admitted onto a national register called the Midwives Roll in order to practise. This photo shows two midwives working at the lying-in hospital in Lambeth (the building can still be seen today). Hospitals were slowly becoming more common and safer after the discovery of antiseptics and were useful places to train both midwives and doctors. The richest families still preferred to give birth at home with doctors in attendance.
6 of 11
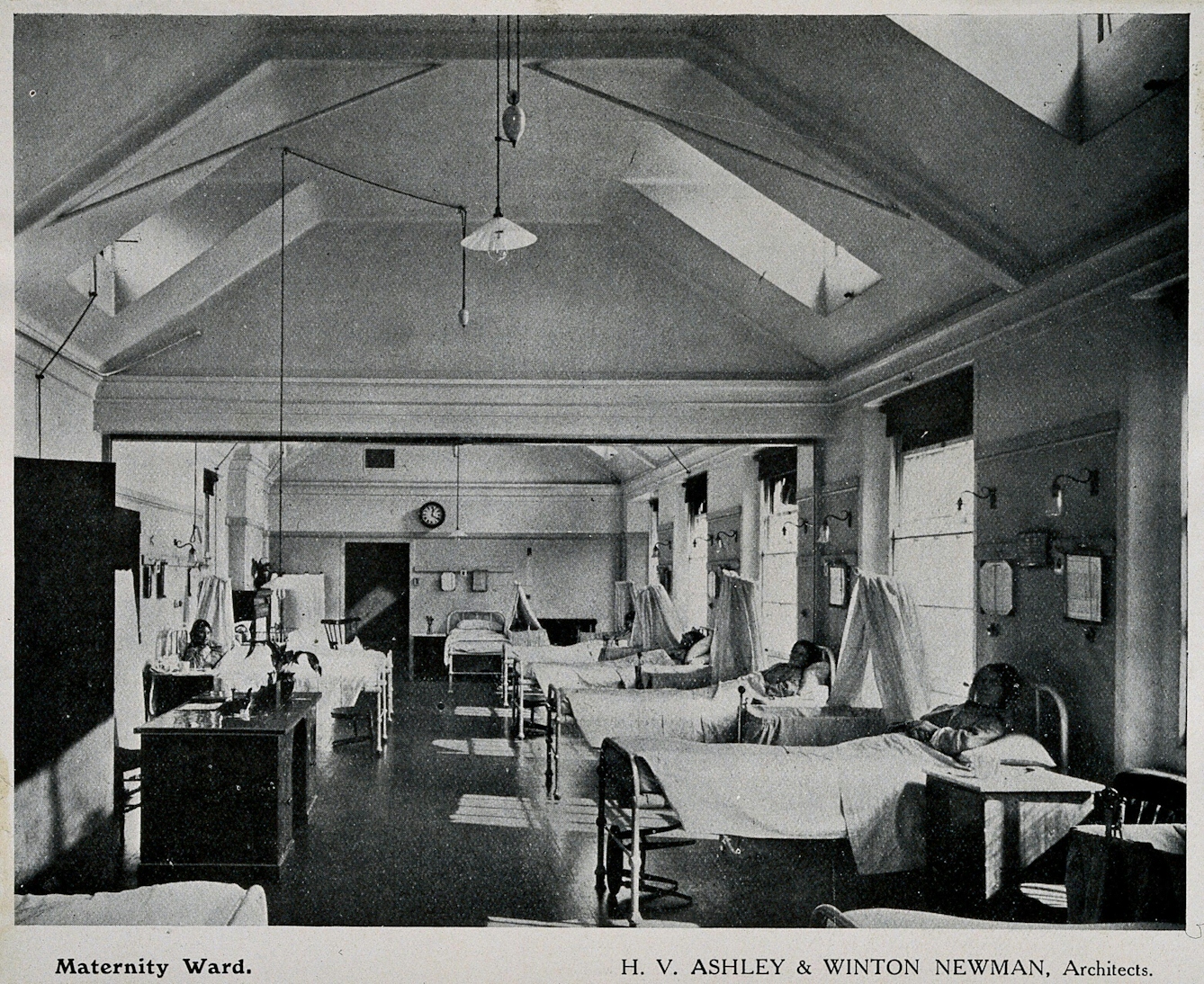
By World War II, hospitals were no longer seen as the most dangerous places to give birth. Antiseptics and, from the 1940s, antibiotics, meant that fatal infections were less common. Pain relief such as nitrous oxide (gas and air) and pethidine were also available to women giving birth in hospital – they were far less likely to be offered for women having home births. The availability of pain relief and the chance to rest for a few days after birth meant that hospital birth was increasingly a positive choice for women. This picture shows how appealing the quiet and clean atmosphere of the ward could be for women who lived in overcrowded, unsanitary areas.

7 of 11
Giving birth in hospital could be a frightening and lonely experience, though. By the 1960s, the majority of births took place in hospital, as government reports argued that it was the safest place to give birth – particularly for babies. Short staffing meant that many women were left alone to labour, without the support of friends and family. Partners were not welcome on delivery suites until the 1970s. Women were encouraged to sacrifice their comfort and wellbeing for the sake of their baby. The hard, uncomfortable birthing bed became a symbol of hospital birth, although some women campaigned for the right to move around in labour and to give birth standing up.

8 of 11
This piece of equipment is an early cardiotocography (CTG) machine used to monitor the foetal heart rate in labour. The use of technology to manage labour and birth exploded in the 1960s and 1970s. Epidural anaesthesia, foetal monitoring, ultrasound scanning and induction of labour all developed during this period. They all required labour and birth to take place in hospital. By the mid-1970s nearly 100 per cent of births took place in hospital.

9 of 11
The image of hospital birth can be one of a grand teaching hospital with long wards and impersonal staff. Although hospital was where nearly all women had their babies in the 1970s and 1980s, not all hospitals were the same. Some were huge places with cutting-edge technology and an array of staff. Others were much more modest maternity homes or GP units like the one in this picture. These were small and local and were usually run by a handful of midwives, with GPs dropping in as required. They were often popular with women, as they offered a halfway house between hospital and home, and a personal touch in contrast to big hospitals. By the mid-1980s they were beginning to disappear, with large hospitals seen as safer and more effective.

10 of 11
Individual women have always wanted and needed different things from their labour and birth experience. Some value the high-tech approach, with pain relief and monitoring available. Others have campaigned for other ways of birthing, including the use of birthing pools, aromatherapy and active birth. Home birth continues to be offered alongside hospital birth and midwifery-led units. Regardless of place of birth, women need kindness, support and companionship during labour and birth.

11 of 11
For women in many countries in the world, there is still little choice about place of birth. Many women give birth without skilled attendance or care, which has significant impacts on their health and wellbeing and that of their babies. Maternal death rates remain high in many countries. This poster reminds us of the basic need that many women still have for simple, safe care.
About the author

Tania Staras
Tania Staras is a midwife and historian currently based at the University of Brighton, where she teaches student midwives. Her research interests focus on histories of midwifery and childbirth.